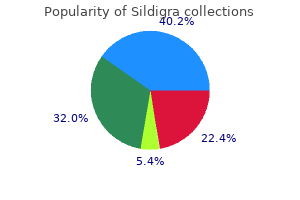
"Discount sildigra 100 mg free shipping, impotence quiz".
By: F. Mufassa, M.B. B.A.O., M.B.B.Ch., Ph.D.
Clinical Director, Harvard Medical School
Their sizes indicate which restriction fragments in the complete digest are next to erectile dysfunction exam what to expect order 100 mg sildigra amex one another in the uncut molecule (Figure 4 erectile dysfunction 18 purchase genuine sildigra. In practice erectile dysfunction injection test order sildigra 25 mg, molecules larger than about 50 kb cannot be resolved efficiently by standard gel electrophoresis. Most, if not all, of the fragments produced in this way will be less than 30 kb in length and easily resolved by agarose gel electrophoresis. Difficulties might arise, however, if an enzyme with a longer recognition sequence is used, such as NotI, which cuts at an eight-nucleotide sequence (see Table 4. It is therefore unlikely that NotI fragments will be separated by standard gel electrophoresis. The limitations of standard gel electrophoresis can be overcome if a more complex electric field is used. Instead of being applied directly along the length of the gel, as in the standard method (Figure 4. This is the key point, because a short molecule can realign faster than a long one, allowing the short molecule to progress toward the bottom of the gel more quickly. This added dimension increases the resolving power of the gel quite dramatically, so that molecules up to several thousand kilobases in length can be separated. This size range includes not only restriction fragments but also the intact chromosomal molecules of many lower eukaryotes, including yeast, several important filamentous fungi, and protozoans such as the malaria parasite Plasmodium falciparum. Within the cell the enzyme carries out the very important function of repairing any discontinuities that may arise in one of the strands of a double-stranded molecule (see Figure 4. A discontinuity is quite simply a position where a phosphodiester bond between adjacent nucleotides is missing (contrast this with a nick, where one or more nucleotides are absent). The chemical reaction involved in ligating two molecules is exactly the same as discontinuity repair, except that two phosphodiester bonds must be made, one for each strand (Figure 4. Although this reaction can be carried out in the test tube, it is not very efficient. This is because the ligase is unable to "catch hold" of the molecule to be ligated, and has to wait for chance associations to bring the ends together. This is because compatible sticky ends can base pair with one another by hydrogen bonding (Figure 4. If the phosphodiester bonds are not synthesized fairly quickly then the sticky ends fall apart again. These transient, base-paired structures do, however, increase the efficiency of ligation by increasing the length of time the ends are in contact with one another. Although a blunt end ligation, this particular reaction can be performed very efficiently because synthetic oligonucleotides, such as linkers, can be made in very large amounts and added into the ligation mixture at a high concentration. If this was the case, the restriction step needed to cleave the linkers and produce the sticky ends would also cleave the blunt-ended molecule (Figure 4. The resulting fragments will have the correct sticky ends, but that is no consolation if the gene contained in the blunt-ended fragment has now been broken into pieces. But unlike linkers, an adaptor is synthesized so that it already has one sticky end (Figure 4. The sticky ends of individual adaptor molecules could base pair with each other to form dimers (Figure 4. The sticky ends could be recreated by digestion with a restriction endonuclease, but that would defeat the purpose of using adaptors in the first place. The answer to the problem lies in the precise chemical structure of the ends of the adaptor molecule. The result is that, although base pairing is always occurring between the sticky ends of adaptor molecules, the association is never stabilized by ligation (Figure 4. If this reaction is carried out in the presence of just one deoxyribonucleotide, a homopolymer tail is produced (Figure 4. In practice, the poly(dG) and poly(dC) tails are not usually exactly the same length, and the base-paired recombinant molecules that result have nicks as well as discontinuities (Figure 4. If the complementary homopolymer tails are longer than about 20 nucleotides, then quite stable base-paired associations are formed. To carry out blunt end ligation with a topoisomerase, a special type of cloning vector is needed.
Splenic marginal zone lymphoma erectile dysfunction diabetes reversible sildigra 50mg fast delivery, second-line (if prior treatment with rituximab) or subsequent therapy in combination with bendamustine for recurrent disease erectile dysfunction journal generic sildigra 25 mg visa, maintenance therapy erectile dysfunction doctor in kuwait purchase 25mg sildigra overnight delivery, or substitute for rituximab in patients experiencing rare complications from rituximab 8. Histologic transformation of marginal zone lymphoma to diffuse large B-cell lymphoma substitute for rituximab in patients experiencing rare complications from rituximab 9. Mantle cell lymphoma, substitute for rituximab in patients experiencing rare complications from rituximab 10. Diffuse large B-cell lymphoma, substitute for rituximab in patients experiencing rare complications from rituximab 11. High-grade B-cell lymphomas, substitute for rituximab in patients experiencing rare complications from rituximab 12. Burkitt lymphoma, substitute for rituximab in patients experiencing rare complications from rituximab 13. Post-transplant lymphoproliferative disorders, substitute for rituximab in patients experiencing rare complications from rituximab 15. The requested medication will be used as a substitute for rituximab in members experiencing rare complications from rituximab such as mucocutaneous reactions including paraneoplastic pemphigus, Stevens-Johnson syndrome, lichenoid dermatitis, vesiculobullous dermatitis, and toxic epidermal necrolysis. The requested medication will be used as second-line or subsequent therapy in combination with bendamustine. The requested medication be used as maintenance therapy when the member has been previously treated with the requested medication and bendamustine. The requested medication is used as a substitute for rituximab in members experiencing rare complications from rituximab such as mucocutaneous reactions including paraneoplastic pemphigus, Stevens-Johnson syndrome, lichenoid dermatitis, vesiculobullous dermatitis, and toxic epidermal necrolysis. Russell-Silver syndrome All other indications are considered experimental/investigational and are not a covered benefit. Pretreatment growth hormone provocative test result(s) (laboratory report or medical record documentation) C. Laboratory-specific values must be provided to determine whether the value is within the normal range. Prader-Willi Syndrome Authorization of 12 months may be granted to members with Prader-Willi syndrome when the following criteria are met: 1. The diagnosis of Prader-Willi syndrome was confirmed by genetic testing demonstrating any of the following: a. Member has a structural abnormality of the hypothalamus or pituitary (refer to Appendix A) and 3 documented pituitary hormone deficiencies (refer to Appendix B). Grinspoon S, Mulligan K for the Department of Health and Human Services Working Group on the Prevention and Treatment of Wasting andWeight Loss. Caremark Clinical Programs Review: Focus on growth hormones, growth hormone releasing hormone, Increlex, Somavert. A review of the effects of therapy on growth and bone mineralization in children with congenital adrenal hyperplasia. Treatment with growth hormone and luteinizing hormone releasing hormone analog improves final adult height in children with congenital adrenal hyperplasia. Growth hormone treatment improves growth and clinical status in prepubertal children with cystic fibrosis: results of a multicenter randomized controlled trial. Growth hormone improves clinical status in prepubertal children with cystic fibrosis: Results of a randomized controlled clinical trial. Growth hormone treatment enhances nutrition and growth in children with cystic fibrosis receiving enteral nutrition. Medical guidelines for clinical practice for growth hormone use in adults and children 2003 Update. National Institute for Clinical Excellence: Guidance on the use of human growth hormone (somatropin) for the treatment of growth failure in children. Update of Guidelines for the Use of Growth Hormone in Children: the Lawson Wilkins Pediatric Endocrinology Society Drug and Therapeutics Committee. Guidelines for growth hormone and insulin-like growth factor-I treatment in children and adolescents: growth hormone deficiency, idiopathic short stature, and primary insulin-like growth factor-I deficiency. Growth Hormone Usage in Short Children: American Association of Clinical Endocrinologists Position Statement. Growth Hormone Research Society workshop summary: consensus guidelines for recombinant human growth hormone therapy in Prader-Willi syndrome. Growth hormone is effective in treatment of short stature associated with short stature homeobox-containing gene deficiency: two-year results of a randomized, controlled, multicenter trial.
Medications to erectile dysfunction new treatments cheap sildigra 100mg on-line be available at bedside include extra analgesics/sedation (morphine erectile dysfunction treatment options in india best 50 mg sildigra, fentanyl erectile dysfunction causes weed sildigra 50 mg with visa, midazolam), normal saline, 5% albumin. Discuss with Surgery and Anesthesia teams any specific needs for other blood products, medications or special equipment. Typically a bolus of 100 mg/kg will be given 30 minutes before incision and continued as an infusion of 30 mg/kg/hr. Pulmonary hypertension associated with acute or chronic lung diseases in the preterm and term neonate and infant. Systematic review and meta-analysis of clinical outcomes of early caffeine therapy in preterm neonates. Early pulmonary vascular disease in preterm infants at risk for bronchopulmonary dysplasia. Do not do a "trial off" during Amicar infusion or for 12 hours after discontinuation. Guidelines for Acute Care of the Neonate, Edition 26, 201819 37 Section 2-Respiratory Care Section of Neonatology, Department of Pediatrics, Baylor College of Medicine 15. Part 7: Neonatal Resuscitation: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Early administration of inhaled corticosteroids for preventing chronic lung disease in very low birth weight preterm neonates. Valdes Section 3-Cardiac Care Section of Neonatology, Department of Pediatrics, Baylor College of Medicine 3. One of the most complex adaptations is the transition from the fetal to the postnatal circulatory pattern. Gas exchange in the fetus occurs in the placenta, an organ of high flow and low resistance, which receives 50-55% of the fetal cardiac output. Crossing the placenta - Maternal nutrients and other · components cross the placental barrier, via simple or facilitated diffusion, active transport, bulk flow, pinocytosis, or breaks in the three tissue layers within the villus in order to reach fetal blood. Congenital diseases of the heart: clinical-physiological considerations by by Rudolph, Abraham, M. Reproduced with permission of Wiley-Blackwell via Copyright Clearance Center, Inc. Oxygenated blood (PaO2 30 mmHg, SaO2 70%) leaves the placenta through the single umbilical vein. It then bypasses the hepatic vasculature and right heart via fetal shunts (ductus venous, foramen ovale), ensuring the blood stays oxygen-rich as it enters the left heart. This arrangement allows the left heart, which provides one-third of the fetal cardiac output, to preferentially pump this oxygenated blood to the brain, myocardium, and peripheral circulation. Figure 3-1 depicts the distribution of fetal blood flow as percentages of the combined fetal cardiac output. The right heart, provides two-thirds of the fetal cardiac output, as it receives deoxygenated blood from the venae cavae, diverts it away from the lungs and across the ductus arteriosus to the descending aorta and to umbilical arteries (PaO2 15 mmHg, SaO2 30%) for reoxygenation in the placenta. Additionally, fetal hypoxia is also a contributing stimulus to the production of prostaglandin E, which maintains ductal patency. As left-sided heart pressures increase and right-sided pressures fall, the foramen ovale closes. The end result is an oxygenator (pulmonary circulation) that is in series with the systemic circulation. Under normal conditions, this process of transition is largely completed within 24 hours. During this time, the function of a circulation in series is disturbed by persistent patency of the ductus arteriosus and foramen ovale, and the potential for abnormal mixing of blood between the systemic and pulmonary circulations. Blood may flow either along the pulmonary-to-systemic circuit (right-to-left shunt) and cause hypoxemia or it may flow along the systemic-to-pulmonary circuit (left-to-right shunt) and cause pulmonary congestion. The direction of shunting is primarily driven by the relationship between systemic and pulmonary vascular resistance. The main determinants of resistance to blood flow in the pulmonary circuit are degree of alveolar hypoxia, and size of the vascular bed, (reduced size can result in an increase in resistance as seen in patients with hypoplastic lungs). Transitional Circulation Guidelines for Acute Care of the Neonate, Edition 26, 201819 Section of Neonatology, Department of Pediatrics, Baylor College of Medicine Section 3-Cardiac Care Table 3-1.
Nonetheless erectile dysfunction treatment by acupuncture order sildigra online now, you have a responsibility to erectile dysfunction urinary tract infection proven 50mg sildigra educate and refer the driver for Page 24 of 260 further evaluation if you suspect an undiagnosed or worsening medical problem erectile dysfunction shakes menu best purchase for sildigra. Seek further testing/evaluations for those medical conditions of which you are unsure. Refer the driver to his/her personal health-care provider for diagnosis and treatment of potential medical conditions discovered during your examination. Promote public safety by educating the driver about: o Side effects caused by the use of prescription and/or over-the-counter medications. Medical Examination Report Form - Overview As a medical examiner, you must perform the driver physical examination and record the findings in accordance with the instructions on the Medical Examination Report form. The purpose of this overview is to familiarize you with the sections and data elements on the Medical Examination Report form, including, but not limited to: · · · Organization of the form. You are encouraged to have a copy of the Medical Examination Report form for reference as you review the remaining topics. Type of Certificate - A complete physical examination is required for both a "New Certification" and "Recertification. Health History the Driver completes and signs section 2, and the Medical Examiner reviews and adds comments: Figure 5 - Medical Examination Report Form: Health History Health History - Driver Instructions the driver is instructed to indicate either an affirmative or negative history for each statement in the health history by checking either the "Yes" or "No" box. The driver is also instructed to provide additional information for "Yes" responses, including: · · · · · Onset date. Medications used regularly or recently, including prescriptions, over-the-counter, and herbal supplements. Health History - Driver Signature Verify that the Driver signs Medical Examination Report Form: Figure 6 - Medical Examination Report Form: Driver Signature Page 27 of 260 By signing the Medical Examination Report form, the driver: · · Certifies that information is "complete and true. Regulations - You must review and discuss with the driver any "Yes" answers For each "Yes" answer: · · · · Ask about history, diagnosis, treatment, and response to treatment. Obtain additional tests or consultations, as necessary, to adequately assess the medical fitness of the driver. Review and discuss driver response to treatment and medications currently or recently used, including over-the-counter medications, and discuss any potential effects and side effects that may interfere with driving. As needed, you should also educate the driver regarding drug interactions with other prescription and nonprescription drugs and alcohol. Recommendations - Questions that you may ask include: Does the driver have: · Symptoms that interfere with safe driving because of: o o o o · Frequency? Limitations that interfere with safe driving because of: o Degree of limitation present? Page 28 of 260 Health History (Column 1) - Overview In addition to the guidance provided in the section above, directions specific to each category in Column 1 for each "Yes" answer are listed below. Any illness or injury in the last 5 years A driver must report any condition for which he/she is currently under treatment. The driver is also asked to report any illness/injury he/she has sustained within the last 5 years, whether or not currently under treatment. Seizures, epilepsy Ask questions to ascertain whether the driver has a diagnosis of epilepsy (two or more unprovoked seizures), or whether the driver has had one seizure. Gather information regarding type of seizure, duration, frequency of seizure activity, and date of last seizure. Eye disorders or impaired vision (except corrective lenses) Ask about changes in vision, diagnosis of eye disorder, and diagnoses commonly associated with secondary eye changes that interfere with driving. Complaints of glare or near-crashes are driver responses that may be the first warning signs of an eye disorder that interferes with safe driving. Ear disorders, loss of hearing or balance Ask about changes in hearing, ringing in the ears, difficulties with balance, or dizziness. Loss of balance while performing nondriving tasks can lead to serious injury of the driver. Obtain heart surgery information, including such pertinent operative reports as copies of the original cardiac catheterization report, Page 29 of 260 stress tests, worksheets, and original tracings, as needed, to adequately assess medical fitness for duty.