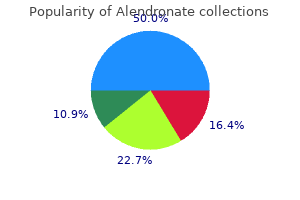
"Alendronate 35 mg online, menstruation symptoms".
By: W. Xardas, MD
Clinical Director, Albany Medical College
The osteoporotic bones contain an abnormal tissue structure since they have lost mass or density breast cancer xrays buy alendronate on line amex. Osteoporosis is a common disease and approximately 54 million people inAmerica have the disease and reduced bone mass breast cancer socks buy alendronate 35 mg with mastercard. Althoughthediseaseaffectspeopleof all races menstrual cycle day 4 alendronate 35mg visa, the white andAsian women especially those whoarepastmenopauseareatthehighestrisk. The disease causes loss of height in somepatientsandhunchedorstoopedpostureifbonesof thespineorvertebraeareaffected. Itlimitsthemobility ofpatientsleadingtoisolationanddepressionandalso complications related to the disease and surgery cause deathofapproximately20%ofolderpeoplewhobreak their hips 15. Osteoporosis is costly as it accounts for about2millionbrokenbonesandrelatedcostsofabout $19billionannually 8. Some medicines like aluminum-containing antacids, cancer chemotherapeuticdrugs,steroidmedicines,andlithium also cause bone loss and osteoporosis 4. The disease is also more common in individuals whose bodieshavetoolittleortoomuchofspecifichormones likethethyroidandsexhormones. Bone lossandosteoporosiscanbepreventedandweakbones strengthened through medications, weight-bearing exercise,andhealthydiet 23. First, alteredlevelsofserotoninareassociatedwiththedisease astheproductionofelevatedlevelsinthegastrointestinal tractisthepossiblecauseforosteoporosisasitdecreases bone formation 5. Second,higherlevels Indian Journal of Public Health Research & Development, January 2019, Vol. The incidence of fracture among patients with inflammatory bowel disease: a population-based cohort study. Incidence and economic burden of osteoporosisrelated fractures intheUnited States,20052025. Wefound outthatosteoporosisdiagnosiswasidentifiedin23,287 patients and concurrent fracture diagnoses in 3,093 cases. Irritablebowelsyndrome: epidemiology, natural history, health care seeking andemergingriskfactors. Irritable bowel syndrome in the United States: prevalence, symptompatternsandimpact. Metabolic 918 Indian Journal of Public Health Research & Development, January 2019, Vol. Risk factors for irritable bowel syndrome: role of analgesics and food sensitivities. Global prevalence of and risk factors for irritable bowel syndrome: a metaanalysis. Determinants of bone mineral density and risk factors for osteoporosis in healthy elderly women. Irritablebowel syndrome in a community: symptom subgroups, risk factors, and health care utilization. Recurrentaphthousstomatitislesionsare likely to occur on non-keratinized, non-attached oral mucosa (1). VitaminD suppressesantigenpresentation,proliferationofT-cells and production of antibodies by B-cells. Theaccountofsecreted cytokines is altered by vitamin D; production of Th1 cytokinetypeisdecreasedandproductionofTh2typeis increased. Theimmunomodulatoryeffectofthisvitamin has raised an interest in its possible role in aetiology of immunodependent entities. Onesuchoutcomeistheenhanced production of antibacterial proteins: cathelicidins and defensins 18. The study group is selected consecutively from the patients attending to theoralmedicineclinicofcollegeofdentistry,Baghdad University between March to April 2018. Separated serums will be collected and stored at 20 C until laboratorytestswillbeperformed. Statistical analysis: Statistical analysis were Indian Journal of Public Health Research & Development, January 2019, Vol.
Omega-3 Fatty Acids (Alpha-Linolenic Acid). Alendronate.
- Reducing the risk of hardening of the arteries (atherosclerosis).
- High blood pressure.
- What other names is Alpha-linolenic Acid known by?
- Dosing considerations for Alpha-linolenic Acid.
- Reducing the risk of heart disease and heart attacks.
- Are there safety concerns?
- Reducing the risk of pneumonia.
- How does Alpha-linolenic Acid work?
- What is Alpha-linolenic Acid?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96991
Lightning Strike-Patients who require critical care after a lightning strike usually are admitted for complications or simply for cardiac monitoring breast cancer kd shoes order alendronate in united states online. Lightning victims may present with paraplegia or quadriplegia that resolves over several hours pregnancy first trimester symptoms purchase alendronate online now. In cases of prolonged paresis womens health program order 35mg alendronate otc, imaging studies should be obtained to rule out a spinal injury. Initial hypertension usually resolves spontaneously and does not require treatment. Lightning victims may have a number of associated findings related to blunt trauma sustained at the time of impact. Burns may be present but are superficial in most patients and often require only superficial wound care. Unlike those who have sustained electrical injuries, patients with lightning injuries rarely develop myoglobinuria. Adequate urine output must be ensured to prevent renal failure from myoglobinuria. Mannitol may be give as a bolus (1 g/kg) and then as an infusion to maintain an osmotic diuresis as long as the urine contains myoglobin (positive hemoglobin nitrotoluidine test). Sodium bicarbonate may be added to alkalinize the urine and prevent the precipitation of acid hematin. Arrhythmias-After initial stabilization, the most immediate risk is from cardiac arrhythmia, particularly when the electric current has passed through the thorax. However, most arrhythmias are selflimited and infrequently cause hemodynamic abnormalities. Atrial fibrillation occurs occasionally and usually will convert without treatment. Myocardial infarction is unusual, but patients with high-voltage injuries may sustain direct myocardial damage. In these patients, close monitoring of fluid therapy may be necessary to prevent pulmonary edema. Neurologic Sequelae-More than half of patients with severe electrical injury develop loss of consciousness, but full recovery usually ensues. Neurologic sequelae sometimes are delayed and may develop days to years after the injury. Ionizing radiation can be either electromagnetic (eg, xrays and gamma rays) or particulate (eg, electrons, protons, and neutrons). The power of penetration of these particles is determined by the energy they carry. High-energy particles can travel deep into the body and cause severe damage to tissues. Very high radiation doses will disrupt cell metabolism and result in rapid cell death. At that time, cell division may be arrested, or the daughter cells may lack essential genetic material and become nonfunctional. This may result in no observable effect or in subsequent malignant transformation. With very high levels of exposure, dysfunction of the cardiovascular and central nervous systems is also observed, most likely resulting from direct organ injury. Peripheral nerve injuries and motor neuropathies result from demyelinization, vacuolization, gliosis, and perivascular hemorrhage. Burns-Most critical care required by victims of electrical injury relates to burns. Treatment: Lightning Strikes the most severe complication of lightning injury is respiratory arrest caused by depression of the respiratory control center. Surviving victims of lightning strikes tend to have fewer complications than patients with electrical injury. Early emergency resuscitation usually stabilizes these patients to the point that only observation is necessary. Most patients will be confused and have anterograde amnesia covering a period of several days after the incident. It is defined as that quantity of radiation that deposits 100 ergs of energy per gram of tissue.
Theoretically pregnancy hospital bag checklist order 35mg alendronate amex, increased work of breathing should be a good predictor of the success of weaning from mechanical ventilation and could provide a guide to women's health center valdosta discount alendronate 35 mg line maximizing respiratory Intrathoracic (Intraesophageal) Pressure Intrathoracic pressure requires a pressure sensor within the chest-almost always a balloon placed in the lower third of the esophagus and connected to menopause guidelines purchase online alendronate a suitable manometer. Care must be taken to position the balloon within the chest and not in the stomach. A potential use is to "correct" pulmonary artery or pulmonary artery wedge pressures for large swings in intrathoracic pressure during the respiratory cycle. For critically ill patients, this requires a pulmonary artery catheter, and most commonly it has been an intermittent calculation. However, with continuous cardiac output technology, continuous mixed venous oximetry, and arterial pulse oximetry, a continuously calculated oxygen consumption is now possible. Calculation of oxygen consumption by the Fick equation also has significant inherent inexactness. Intermittent thermodilution measurements of cardiac output have significant variance, as do measurements of arterial and venous saturation, as well as hemoglobin. Any errors in these measurements are increased geometrically during calculation of oxygen consumption-so-called mathematical coupling. However, the importance of this limitation to the accuracy of this methodology in clinical practice is a matter of controversy. However, it is not clear that providing "supranormal" oxygen delivery improves outcome for critically ill patients with shock, sepsis, trauma, or hemorrhage. One important exception is during the early phase of sepsis and septic shock, in which attention to oxygen delivery (assessed using central venous oxygen saturation) increases survival. There are insufficient outcome data supporting routine use of indirect calorimetry, but numerous studies have pointed out that, without direct measurements, patients are often under- or overfed in comparison with their actual needs. As technology advances and as fiscal realities increase the incentive to control health care spending, increased regionalization will result in transport of the critically ill to the hospital that can best manage the patient. Lessening the need for duplicate resources by regionalization of specialized health care services may achieve optimal patient outcomes at minimal costs. Repatriation of health plan participants with their primary care providers has led to a dramatic increase in interfacility transport of persons requiring hospitalization or extended emergency evaluation. Management of resource-intensive critical illness in specialized regional centers has been shown to improve medical outcomes and cost-effectiveness. Most studies support the concept that patient volume in tertiary care centers (Table 91) leads to better patient outcomes because staffs of these centers maintain high experience and proficiency levels. With medical evidence strongly supporting regionalized medical specialty centers, methods for transport of patients to these centers must be developed using practices based on the best scientific and management evidence. For interfacility transfers, there are no standard guidelines regarding which patients may be transferred solely with paramedics, which require a nurse in attendance, and which require a physician in attendance. Local regulations may restrict the role of paramedics, who should not, for example, give medications or manipulate unfamiliar equipment such as ventilators unless they have documented evidence of training and competence. The scope of such training may be limited by the paramedic licensing or certification board. There are no national data on overall transport volumes or team composition within transport systems. Published guidelines recommend that a minimum of two medically qualified people in addition to vehicle operators accompany a critically ill patient. In urban areas, ground transport is most common; in rural areas, air transport is more often required because of the distances and the difficulties of road travel. This scope of practice limits what the individual may or may not do during the transport process. Many critical care transport programs that have physicians on board transport vehicles are using physicians who are still in training-there is little information about whether the level of experience of the physicians is a factor in outcome. Many programs ascribe considerable value to the presence of physicians; this despite the fact that only 11% of programs fly with physicians on board. Burn injuries Trauma High-risk blunt and penetrating injuries Neurologic injuries Vascular injuries Complex orthopedic injuries Pediatric-age trauma Oro-maxillary-facial injuries Obstetric, high-risk Neonatal care Pediatric critical care Cardiac Invasive coronary revascularization High-risk cardiac care Cerebrovascular ("stroke") management Rehabilitation, intensive Table 92. Favoring ground ambulance Ambulance staffed by critical care team Ambulance equipped appropriately Patient location accessible to ground transport Ambulance can be spared for use within the local system Geography allows ground transport Favoring helicopter transport Transport distance 30180 miles Important to minimize transport time Helicopter staffed by critical care team Helicopter equipped appropriately Patient location and receiving location accessible to helicopter landing and takeoff Allowable weather conditions Patient/equipment weight allows use of available helicopter Favoring fixed-wing aircraft Transport distance over 100150 miles Important to minimize transport time Aircraft staffed by critical care team Aircraft equipped appropriately Patient location and receiving location accessible to an airport Allowable weather conditions Patient/equipment weight allows use of available aircraft Critical care transport available for moving patient to and from landing sites Appropriately educated and monitored nonphysicians can use paralytic pharmacologic agents and perform intubation, cricothyrotomy, and tube thoracostomy safely; nurses or respiratory therapists may be more familiar with ventilators than a physician.
Shearing stress from rapid deceleration has been regarded as the primary biomechanism of this injury premier women's health zephyrhills order alendronate with a visa, but recent evidence suggests that lateral-impact collision forces with simultaneous acceleration of the victim and increased hydrostatic pressure within the aorta also may be important mechanisms women's health center beverly ma order alendronate on line amex. Early symptomatic presentation usually is exsanguinating rupture or distal dissection women's health clinic winnipeg order discount alendronate online, whereas late presentation is in the form of a pseudoaneurysm. Aortic transection occasionally is due to penetrating violent injury or to iatrogenic trauma during cardiac or other surgery. Aortic Dissection-Aortic and other great vessel dissections represent pathologic separation of the vessel layers, thereby creating a true lumen and a false one. Mechanistically, rupture of the vasa vasorum is probably the most important inciting event. It is not clear whether spontaneous bleeding into the aortic wall (ie, intramural hematoma) may cause aortic dissection. Once the intimal tear occurs, there is progressive separation of the adventitia and the intima. This separation typically propagates distally but occasionally may extend proximally. As the separation extends, branch vessels may be themselves dissected, occluded, or completely unaffected depending on the location and extent of the aortic dissection. The dissection then either reenters the true lumen via a second or third tear in the intima or creates a blind pouch. These "neostructures" then may remain permanently patent because of continued flow down the false channel, or they may thrombose owing to stasis. These dynamics of aortic dissection are a function of the balance between tissue strength and continued shear forces. Shear forces, in turn, are determined by blood pressure, change in blood pressure with time (dP/dT), size and location of the intimal tear, and blood vessel diameter. Two classification schemes are used commonly, based on the location and extent of dissection-the Stanford and DeBakey classifications. A Stanford type A dissection begins in the ascending or transverse aorta with variable amounts of aortic involvement. Type B dissections begin distal to the takeoff of the last great vessel, usually the left subclavian artery. By comparison, a type I DeBakey lesion is analogous to an extensive Stanford type A dissection. Both begin in the ascending aorta and extend across the arch and down the descending aorta. These classification schemes are vital to management and prognosis, with particular emphasis on identifying involvement of the ascending aorta. Type A dissections have an 80% mortality within 48 hours without surgical treatment, whereas selected type B dissections frequently can be managed medically with only a 10% mortality at 30 days. These vastly different outcomes are based primarily on the proximity of type A dissections to vital structures, including the heart, coronary arteries, aortic valve, and carotid vessels. Myocardial infarction, acute aortic insufficiency, intrapericardial rupture causing tamponade, and stroke are all frequent consequences of proximal dissections. The surgical risks and adverse effects of therapy multiply with extent and acuity of the disease process. Symptoms and Signs-Any patient with significant chest pain should be assumed to have an aortic catastrophe until another cause is established. Discrepancies in peripheral pulses and blood pressures occur frequently, particularly in the presence of aortic valve insufficiency. Changes in pulse contour or distribution may help to localize the extent of a dissection or transection. Dissections in particular-and sometimes aneurysms- have myriad presentations, making them a diagnostic challenge. By far the most common symptom accompanying aneurysms, transections, and dissections is chest pain, usually sharp and, less frequently, tearing or ripping, with radiation to the back or abdomen. Aneurysms may present with pressure symptoms related to the recurrent laryngeal nerve, great veins, trachea, esophagus, or chest wall. Significantly, aneurysms may be asymptomatic until they rupture and present with circulatory collapse. Any number of end organs may become ischemic temporarily or permanently with their own characteristic symptoms. Temporary neurologic findings are particularly common, but any vascular organ can present with initial or subsequent ischemia.