"Buy discount septra 480mg on-line, symptoms 28 weeks pregnant".
By: K. Garik, M.A.S., M.D.
Associate Professor, Donald and Barbara School of Medicine at Hofstra/Northwell
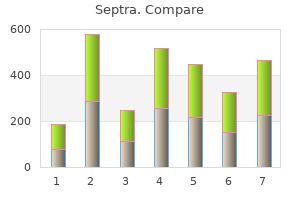
Therefore treatment 2 order 480mg septra otc, although there have been some remarkable successes in scientific investigation aimed at elucidating fundamental sleep physiology and biology symptoms 5dp5dt cheap septra 480 mg fast delivery. Fundamental scientific discoveries play critical roles in galvanizing interest in any scientific discipline medications buy discount septra line. Recruiting and retaining trainees in somnology and sleep medicine competes with other more established fields, many of which have made highly publicized advances, enjoy widespread respect across medical centers, and are more established as an academic discipline. Investigators, particularly new ones who commit to interdisciplinary sleep-related research, are challenged to prove their value in academic medical centers that are accustomed to recognizing and rewarding individuals with "departmentally" defined research foci. Resource allocation needed to support new investigators may require complex negotiations among academic departments, which may deter new investigators or otherwise limit their access to needed support. In addition, identification of optimal mentoring relationships, critical for career development, will likely require sustained relationships among individuals with competing institutional commitments. Increasing fiscal pressures and, for physicians, demands to spend more time on clinical services, are threats to protected time critical for career development. New investigators are also often burdened with substantial debt from school loans, providing disincentives to participate in prolonged postdoctorate training. Programs have been developed with the aims of attracting new trainees and developing the research and academic skills, and supporting their transition to independent and externally funded investigators (K01, K02, K08, K23, and K25). National Research Service Award Institutional Training Grants (T32) provide institutions with funds to support the training of individual postdoctoral candidates. To limit the number of grants that were not relevant to somnology or sleep disorders, the committee included only grants in which the key words appeared in both the thesaurus terms and the abstract and not the abstract alone. Analysis of the number of sleep-related T and F awards shows an increase between 2000 and 2004 (Figure 7-2). However, the number of K awards decreased over the same time period and a larger proportion went to a smaller group of academic institutions. Three institutions, Harvard University, University of Pennsylvania, and University of Pittsburgh, accounted for 27 percent of all sleep-related T, K, and F grants received in 2000, 35 percent in 2004. The same three institutions received 29 percent of all K awards in 2000, and 46 percent in 2004. This may reflect the extensive development of these programs and concentration of senior investigators. In general, for any given award category, with few exceptions no more than one new career development award was granted in any given year between 2000 and 2004. Since 2000, investment in career development awards for clinical scientists, K08 and K23, has varied. Although there has been greater investment in the K23 series, it is still minimal with five new awards in 2003 by four different institutes. There has also been very limited investment in the K07 academic career awards, designed to improve curricula and emphasize development of scientist leadership skills. Apart from the Sleep Academic Award program, there has been very little investment through the K07 mechanism, no new awards were granted in 2003, and only three in 2004. Over the 5-year period between 2000 and 2004, there has been even less investment in career development awards for mentored research (K01), independent scientists (K02), and senior scientists (K05). All three of these mechanisms historically have been used to support basic research. In 2004, these numbers have decreased to two K01 awards, two K02 awards, and one K05 award. Although the decrease in career development awards is dramatic, it is important to note that over the same period, there has been an increase in fellowship awards (Appendix I). The underlying reasons may be multiple, including poor or low numbers of applications, insufficient sleep-related research expertise on study sections (which is also partially affected by a limited number of senior members of the field), and lack of awareness of the extent of the problem. Further, mechanisms need to be developed to enable all institutes contributing to a joint effort to be acknowledged in congressional goals for new grants. Each initiative is designed to facilitate postdoctoral fellows into independent faculty positions. The initial phase (K99) is a 1- to 2-year mentored period designed to allow investigators to complete their supervised research work, publish results, and search for an independent faculty position.
High glucose concentration causes impairment in cell growth and production of growth factors and the occurrence of genes which will ultimately increase the extracellular matrix medications gout buy 480 mg septra amex. Also with inhibition of collagenases synthesis causes decreased extracellular matrix removal medicine youth lyrics cheap 480 mg septra with mastercard. Long-term hyperglycemia causes structural changes in some proteins that biological activity of these new compounds are high symptoms lung cancer order septra 480mg, like HbA1c. Protein kinase C provides an important role in cell proliferation and differentiation, and apoptosis. This enzyme increases extracellular matrix and cytokines and production of endothelin. This changes cause thickening of the glomerular basement membrane and obstruction of arteries and increased glomerular permeability. Another important enzyme in the pathogenesis of diabetic nephropathy is aldose reductase. Long-term hyperglycemia increases the enzyme activity and sorbitol production, which increases the extracellular matrix. Approximately after 3 to 5 years hyalinization of the afferent and efferent arterioles is seen (10). Increasing mesangium volume is seen about 3 to 5 years after diabetes onset, which sometimes reaches 15 years (11). In about half of patients glomerular sclerosis has nodular pattern which is known as Kimmelstiel-Wilson nodules that shows severe glomerular sclerosis. The main pathological lesions that lead to clinical albuminuria and nephropathy is increased mesangial matrix. Mesangial matrix expansion strongly increases the development of systemic hypertension and urinary albumin excretion (12,13). Another important factor in the development of glomerular lesions is hemodynamic derangements. Auto-regulation of renal blood flow is impaired in diabetic nephropathy, so abnormal dilation of afferent arteriole leads to increased glomerular filtration and this can lead to glomerular sclerosis in long term. After developing sclerosis blood flow in remaining intact glomeruli increases and causes rise in glomerular pressure so eventually sclerosis. Systemic blood pressure can also directly transfer to the glomeruli and causes glomerular sclerosis. In type 1 diabetes with microalbuminuria, systemic blood pressure will begin to increases, although it may still be within normal range. Many patients with type 2 diabetes also have essential hypertension that increases after beginning of renal lesions. Journal of Renal Injury Prevention, Volume 2, Number 2, June 2013 Genetics Many patients with long-term hyperglycemia have no nephropathy while others with not very long disease course have clinical nephropathy. Risk of diabetic nephropathy increases in type 1 and type 2 diabetic patients with a history of diabetic nephropathy in one of their first degree relatives. One of the genetic factors is angiotensin type 2 receptor gene on the X chromosome. Male patients with type 1 diabetes who are homozygous for the gene have lower glomerular filtration than heterozygous groups (18). Diabetic patients who have a family history of hypertension or cardiovascular disease are more likely to develop nephropathy. Also the polymorphisms of genes related to insulin resistance plays a role in the development of diabetic nephropathy. Screening There are various methods for screening of diabetic nephropathy in patients. It actually starts to prove microalbuminuria, to prevent its progress toward macroalbuminuria (clinical nephropathy), or even turn it into normoalbuminuria status. Microalbuminuria defines as urinary excretion of 30-300 mg of albumin in the 24 hours urine collection continuously. Macroalbuminuria of clinical nephropathy is when albumin excretion in 24 hours urinary collection be greater than 300 mg continuously (Table 1). Some evidence indicates that the onset of type 1 diabetes before puberty may play a role in creating microvascular complications including nephropathy. Therefore, clinical judgment about when to start screening on every patient should be considered individually.
Buy septra 480 mg lowest price. SHINee - Everybody (Piano Duet).
The fibres of pain and thermal sensation cross the midline in the anterior white commissure and ascend up as lateral part of anterolateral spinothalamic tract symptoms 6 days post iui purchase septra 480mg amex. Anterior Spinocerebellar Tract this tract carries unconscious proprioception from lower limb as a whole medicine park lodging buy septra mastercard. Axons from spinal border cells cross the midline and enter the cerebellum through the superior cerebellar peduncle and most of the fibres recross in the cerebellum treatment uveitis discount 480 mg septra visa. Clinical Anatomy A unilateral lesion of spinal cord will show bilateral ataxia of lower limbs, if the ventral spinocerebellar tract (carrying contralateral proprioceptive impulses) and dorsal spinocerebellar tract (carrying ipsilateral proprioceptive impulses) are affected. The upper limb equivalent of posterior spinocerebellar tract is cuneocerebellar tract (which lies in the medulla oblongata). The upper limb equivalent of ventral spinocerebellar tract is rostral spinocerebellar tract arising from diffuse neurons in the base of the posterior horn of cervical part of spinal cord. Fasciculi gracilis and cuneatus decussate at medulla; spinothalamic tract decussates at spinal cord. Hence, spinal cord lesions cause ipsilateral loss of fine senses and contralateral loss of pain. A lesion anywhere in the brainstem or higher will cause contralateral loss of both senses-a great localizing sign. Clinical Anatomy Disorders of equilibrium: Inability to maintain the equilibrium of the body, while standing or while walking, is referred to as ataxia. This may occur as a result of interruption of afferent proprioceptive pathways, i. The fibres starting from sensory cortex influence sensory input to the central nervous system. A few fibres also arise from association areas of parietal, temporal and occipital lobes. After passing through the internal capsule, the fibres enter the crus cerebri (of the midbrain) and then descend through the ventral part of the pons to enter the pyramids in the upper part of the medulla. Near the lower end of the medulla about 80% of the fibres cross to the opposite side and enter the lateral funiculus of the spinal cord and descend as the lateral corticospinal tract (Figure 3. The corticospinal fibres that do not cross in the pyramidal decussation enter the anterior funiculus of the spinal cord to form the anterior corticospinal tract. On reaching the appropriate level of the spinal cord, many of the fibres of this tract cross the midline (through the anterior white commissure) to reach grey matter on the opposite side of the cord. A few terminate on the same side and are responsible of bilateral activities of the trunk. The fibres of the tract cross to the opposite side of the midbrain and pass through the pons and medulla to enter the lateral funiculus of the spinal cord (Figure 3. The tract terminates in the cervical segments of spinal cord and is facilitatory to flexors of upper limb. Tectospinal Tract the fibres of this tract arise from neurons in the superior colliculus (midbrain). The fibres cross to the opposite side in the midbrain and descend through the pons and medulla into the anterior funiculus of the spinal cord (Figure 3. This tract is responsible for reflex postural movements of neck in response to visual stimuli. Note that the fibres of both the tracts cross to the opposite side in midbrain (in dorsal and ventral tegmental decussations) Clinical Anatomy the cerebral cortex controls voluntary movement through the corticospinal tract. Medial Reticulospinal Tract Fibres arise from the medial part of the reticular formation of pons. The tract is concerned with postural adjustments of the head, trunk and limbs (Figure 3. Extrapyramidal Tracts Descending tracts arising from subcortical centres are called extrapyramidal tracts. Lateral Reticulospinal Tract this tract is constituted by fibres arising in the reticular formation of the medulla oblongata. They descend in the lateral funiculus 50 Textbook of Human Neuroanatomy (Figure 3. Lateral Vestibulospinal Tract the neurons of origin of the lateral vestibulospinal tract lie in the lateral vestibular nucleus located at pontomedullary junction.
Fibres from the tegmentum of the midbrain also reach the hypothalamus through the medial forebrain bundle 300 medications for nclex discount septra line. These are the anterior perforated substance medications errors pictures buy generic septra 480 mg on-line, the septal nuclei symptoms 6 days after conception order septra 480 mg amex, the amygdaloid complex, the hippocampus and the piriform cortex. Others relay in the thalamus (medial, dorsal, and midline nuclei) and reach the hypothalamus through periventricular fibres (so called because they travel just subjacent to the ependyma). The cingulate gyrus may influence the hypothalamus indirectly through the hippocampal formation. Some fibres from the orbital cortex may reach the hypothalamus through the medial forebrain bundle. Connections of Hypothalamus the hypothalamus is concerned with visceral function and is, therefore, connected to other areas having a similar function. These include the various parts of the limbic system, the reticular formation, and autonomic centres in the brainstem and spinal cord (Flowchart 9. Efferent Connections · the hypothalamus sends fibres to autonomic centres in the brainstem and spinal cord. Centres in the brainstem receiving such fibres include the nucleus of the solitary tract, the dorsal nucleus of the vagus, the nucleus ambiguus, and the parabrachial nucleus. Fibres descending to the spinal cord end in neurons in the intermediolateral grey column. It also sends fibres to the hippocampal formation, the septal nuclei, the amygdaloid complex, and the tegmentum of the midbrain, and autonomic centres in the brainstem and spinal cord. These fibres pass through the same bundles that convey afferent fibres from these centres. Fibres from the mamillary body pass through the mamillothalamic tract to reach the anterior nucleus of the thalamus. Fibres from the mamillary nuclei also reach the subthalamic region and the tegmentum. The fibre bundles associated with hypothalamus along with their functions are summarized in Table 9. Functions of Hypothalamus the hypothalamus plays an important role in the control of many functions that are vital for the survival of an animal. In exercising such control, the hypothalamus acts in close coordination with higher centres including the limbic system and the prefrontal cortex and with autonomic centres in the brainstem and spinal cord. The main functions attributed to the hypothalamus are as follows: Control of Hypophysis Cerebri by the Hypothalamus Neurons in some hypothalamic nuclei produce bioactive peptides that are discharged in the neighbourhood of capillaries or, in some cases, into the cerebrospinal fluid. The process of the production of such bioactive substances by neurons (as distinct from release of neurotransmitters at synapses or efferent nerve endings) is referred to as neurosecretion. Regulation of Eating and Drinking Behaviour the hypothalamus is responsible for feelings of hunger and of satiety. A feeding centre has been described in the lateral hypothalamic nucleus and a satiety centre, in the ventromedial nucleus. Regulation of Sexual Activity and Reproduction the hypothalamus controls sexual activity, both in the male and female. It also exerts an effect on gametogenesis, on ovarian and uterine cycles, and on the development of secondary sexual characters. These effects are produced by influencing the secretion of gonadotropic hormones by the hypophysis cerebri. Axons of the paraventricular nucleus descend towards the supraoptic nucleus as the paraventriculohypophyseal tract (Figure 9. They join axons arising from the supraoptic nucleus to form the supraopticohypophyseal tract. The axons of the tract pass down into the infundibulum and from there into the neurohypophysis. Here, the axons branch profusely and end in relation to capillaries around which they release their secretion. Control of Autonomic Activity the hypothalamus exerts an important influence on the activity of the autonomic nervous system and, thus, has considerable effect on cardiovascular, respiratory, and alimentary functions. Sympathetic activity is said to be controlled predominantly by caudal parts of the hypothalamus and parasympathetic activity, by cranial parts. Control of the Adenohypophysis by the Hypothalamus the hypothalamus controls secretion of hormones by the adenohypophysis by producing a number of releasing factors.